English
English
 Deutsch
Deutsch
 الْعَرَبِيَّة
الْعَرَبِيَّة
- Early detection of prostate cancer
- Information about prostate cancer
- Prostate punch biopsy
- Male sexuality
- Diet and nutrition
- Urinary incontinence
- PSA test
- Vasectomy
- Premature ejaculation
- Testosterone
- Malignant bladder tumours
- Testicular tumours
- Renal carcinoma
- Penile carcinoma
- Peyronie’s disease
- Urinary stone disease (urolithiasis)
1.1 What is a prostate?
1.2 What is prostate cancer?
1.3 How does prostate cancer develop?
1.4 What are the symptoms of PCa?
1.5 What metastases can occur?
1.6 How can metastases be detected?
1.7 How can one take precautions?
1.8 Diagnosis of prostate cancer: The PSA value
1.9 Removal of a tissue sample/ prostate lancet biopsy
1.10 Treatment and therapy options
1.11 Patient guide
1.1 What is a prostate?
The prostate is an organ of the male reproductive system and is also called the prostate gland. It is located just below the urinary bladder and above the voluntary sphincter. It forms part of the urethra in this area. The prostate gland forms a large part of the seminal fluid (ejaculate), which it empties into the urethra together with the seminal filaments (spermatozoa) during appropriate sexual stimulation. The spermatozoa pass from the testicles to the prostate via the vas deferens.
1.2 What is prostate cancer?
Das Prostatakarzinom (kurz: PCa) ist der Krebs der Prostata. Dabei handelt es sich um eine bösartige Tumorerkrankung, die vom Drüsengewebe der Prostata ausgeht. Prostatakrebs ist die häufigste Krebserkrankung bei Männern und nach Lungen- und Dickdarmkrebs die dritthäufigste tödliche Krebsart.
1.3 How does the prostate cancer develop?
How prostate cancer develops It is very rare below the age of 45.
The exact cause of prostate cancer is unknown, but a hereditary component seems to play a role. Especially in industrialized countries, the rate of malignant prostate disease is increasing significantly. It is also observed that people with high fat consumption have a significantly increased risk of developing prostate cancer.
Prostate cancer develops as a result of an imbalance of growth factors that control the growth and division of cells in the prostate. Genetic changes in the genetic material of the prostate cells can promote the development of this imbalance. In about 80 percent of cases, prostate cancer develops in the outer area of the prostate, known as the capsule. This can result in tissue changes that can be palpated by the physician as a hard lump during examination from the rectum.
1.4 What are the symptoms of PCa?
In many patients, complaints from prostate cancer, such as back pain, do not occur until an advanced stage.
Back pain may or may not be related to prostate cancer. In the early stages of prostate cancer, symptoms tend to be the exception. In the advanced stage, warning signs such as bladder emptying disorders, bone pain and later weight loss and anemia may occur.
1.5 Which metastases can occur?
As the prostate cancer progresses, the cells can gain access to lymphatic vessels or blood vessels and thus spread throughout the body. Usually, metastases form first in the lymph nodes in the pelvis and only after a delay in other organs.
In certain organs, metastases may spread further down the line and are then called distant metastases. In prostate cancer, distant metastases occur mainly in the bones or lungs.
1.6 How to detect metastases?
An X-ray of the lungs is taken to rule out daughter tumors in the lungs. A so-called whole-body bone scintigram is performed to diagnose possible tumor metastases in the bone. X-rays or ultrasound examinations of the kidneys show whether urinary obstruction (urine stasis in the kidney) has already occurred as a result of the prostate cancer.
Computer tomography or magnetic resonance imaging are expensive examination procedures that usually do not provide the urologist with any important information when deciding on the therapy to be adopted.
1.7 How to provide?
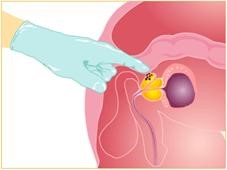
For men from the age of 45, annual screening with prostate palpation and transrectal ultrasound (TRUS) is recommended. If prostate cancer is known in close relatives, screening should start at the age of 40.
In addition, regular measurement of PSA should also be performed to detect changes at an early stage.
If the findings are conspicuous, a punch biopsy is performed to determine whether a carcinoma is present.
1.8 Diagnosis of prostate cancer: the PSA value
Nowadays, the decisive indication of the presence of prostate cancer is provided by a blood test, the determination of the so-called prostate-specific antigen (PSA). The PSA is a substance that is produced exclusively in the prostate gland and to a certain extent enters the bloodstream.
Men without prostate disease usually have a blood concentration of less than 4 nanograms per milliliter (ng/ml). An increase in PSA to values between 4 and 10 ng/ml is considered a gray area: benign prostatic hyperplasia (BPH), prostate inflammation or prostate cancer may be responsible. Values above 10 ng/ml are always suspicious of prostate cancer. However, the final diagnosis of prostate cancer can only be made with the help of a tissue biopsy.
To avoid unnecessary tissue sampling, attempts are now being made to improve the predictive accuracy of this blood test by specific measurements of PSA subunits.
However, if the physician palpates a suspicious lump on the prostate, tissue sampling should always be performed – regardless of the measured PSA value.
Unfortunately, health insurance companies do not cover the costs for the determination of the PSA value in the case of pure screening. There are many opinions whether a PSA determination makes sense or not. After many years of experience, I am of the opinion that PSA control is definitely helpful in the early detection of prostate cancer.
1.9 Removal of a tissue sample/ prostate punch biopsy
If a malignant change in the prostate, i.e. a prostate carcinoma, is suspected, a tissue sample is taken from the prostate under normal blood clotting and antibiotic protection. This examination is known as a prostate tissue biopsy.
The fear that palpation of the prostate or a punch biopsy could trigger an existing cancer or activate a dormant cancer is incorrect and refuted by studies.
The only essential preparation is the need for complete bowel emptying and taking an antibiotic, which begins the day before the biopsy. The antibiotic will be prescribed by us.
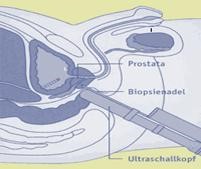
After administration of an antibiotic and after local anesthesia, the tissue samples are taken almost painlessly with the help of a fine needle. The needle is usually advanced into the prostate via the rectum. Usually, an ultrasound probe is now used to selectively remove a tissue sample under visualization. The tissue obtained is reviewed by the pathologist and examined for malignant cells. The result is usually available within a week.
Since prostate cancer can grow in several places in the prostate at the same time and be distributed among many smaller nodes, there is a possibility that these small „cancer nests“ will be missed by the needle. It is therefore sometimes necessary to repeat the tissue sampling after a latency period.
The procedure is performed on an outpatient basis and takes only about ten minutes.
1.10 Treatment and therapy options
Treatment with a chance of cure is only possible if the degenerated tissue has not yet crossed the organ boundaries and there are no metastases.
Therapeutische Optionen sind die Operation mit kompletter Entfernung der Prostata, die man Prostatektomie nennt, die Strahlentherapie und bei Frühformen des Tumors eine aktive Beobachtung („Active Surveillance“). In Active Surveillance, active therapy is used only in the event of an increase in the activity of the cancer.
If the patient decides to undergo surgery, a „minimally invasive“ laparoscopic robot-assisted operation using the DaVinci system is usually performed. This operation represents the most modern surgical therapy currently available.
In addition, many „alternative“ therapeutic options are under trial, but the data to date are not sufficient for any of the therapies to be recommended in terms of the urologic therapy guidelines.
If the diagnosis is not made until symptoms appear, metastasis, i.e. spread of the tumor, may have already occurred.
In these cases, hormone therapy is usually initiated first, as long as the cancer still responds to it. If this is no longer the case, the tumor is said to be „hormone refractory“; in this case, newer substances can be used in studies in addition to various established chemotherapies.
If prostate cancer is diagnosed in patients of advanced age, it can be treated with hormone-suppressive therapy using depot injections.
1.11 Patient guide to locally advanced and metastatic prostate cancer
The guidebook was created by patient representatives and physicians and jointly sponsored by the German Cancer Society (DKG), German Cancer Aid (DKH) and the Association of the Scientific Medical Societies (AWMF). The finished guidebook can be downloaded free of charge from the ÄZQ website (ÄZQ) or ordered as a brochure from German Cancer Aid.